Exploring the Link Between Hard Water and Hair Health
Can hard water cause hair loss? Learn how mineral buildup affects scalp health, weakens hair strands, and discover simple solutions to protect and maintain healthy hair.
Read More
Effective ED Treatment Solutions
"Restore Confidence and Improve Your Performance with Trusted ED Medications. Fast, Discreet Shipping to Your Doorstep from Sanford Pharmacy!"
Read More
Understanding Conditions That May Affect HIV Test Results
Discover which medical conditions and infections can sometimes lead to false-positive HIV test results, why they occur, and how confirmatory testing ensures accurate diagnosis.
Read More
Causes, Relief, and Prevention for Painful Mouth Sores
Learn about the common causes of mouth sores, effective home remedies, treatment options, and practical tips to relieve pain and prevent recurring oral ulcers.
Read More
Recognizing Rabies Early and Protecting Yourself
Learn about rabies symptoms, how the virus spreads, early warning signs, prevention through vaccination, and the importance of immediate treatment after animal bites.
Read More
Featured This Month
Gastrointestinal and Metabolic
How Long Can You Take Prilosec?
 Mikayla
Mikayla
 11 May 2026
11 May 2026
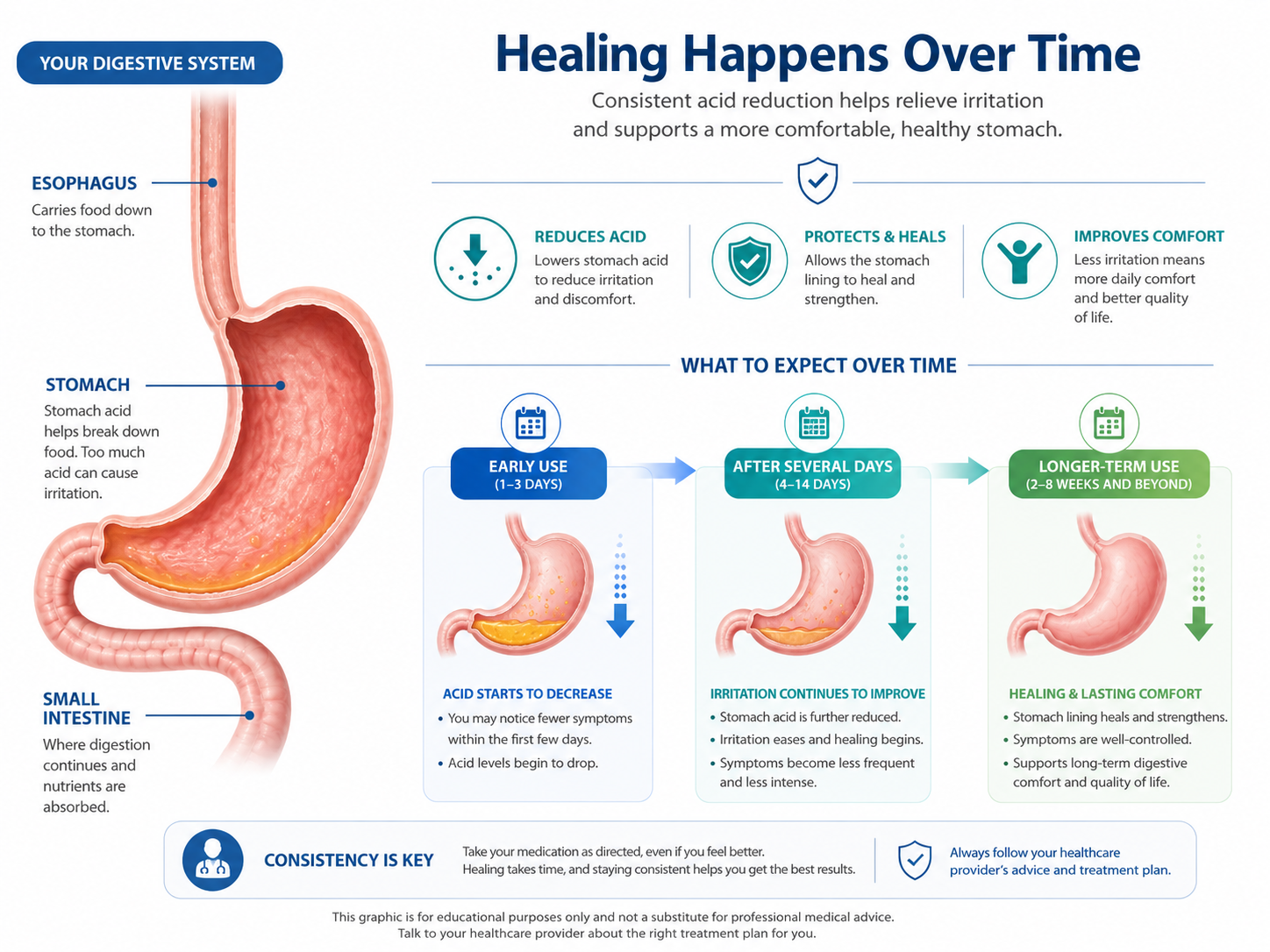
Safe Duration and Long-Term Use of Proton Pump Inhibitors Explained Prilosec isn’t really meant to be something you just take forever without thinking about it. For most people, it’s used for a short stretch — about 14 days if you’re taking it over the counter. If it’s prescribed, that can stretch to 4 to 8 weeks, sometimes longer depending on what’s going on. But the key thing is — the longer you stay on it, the more it should be something you’re checking with a doctor or pharmacist about, not just continuing on your own. What “14 days” actually means (because people misunderstand this a lot) If you look at the box, it says 14 days. Sounds simple. But here’s what that really means in practice: you take it once a day, every day for the full 14 days you don’t just stop when you feel better after a couple days and it’s not something you’re supposed to restart immediately again and again A lot of people take it for 3–4 days, feel better, and stop. Then symptoms come back. That’s because Prilosec doesn’t work like an instant antacid. It builds up its effect. It usually takes a few days (sometimes up to 4) before you feel the full benefit. So the 14 days is more about giving it time to properly settle things down. What happens if symptoms come back This is where things get tricky for a lot of people. You finish the 14 days… and then a week later, heartburn is back. So you take another course. Then maybe another. At that point, it’s less about “how long can I take it” and more about “why do I need it this often?” If you’re repeating those 14-day cycles regularly, it’s usually a sign something needs a closer look. When people are told to take it longer There are definitely situations where Prilosec is used for more than just two weeks. Doctors prescribe it longer for things like: GERD (chronic acid reflux) stomach ulcers duodenal ulcers H. pylori infections (along with antibiotics) In those cases, it’s often: 4 to 8 weeks sometimes longer if symptoms don’t fully settle And sometimes people stay on a lower dose after that. But again — that’s usually planned and monitored, not just continued casually. Why people end up staying on it longer than expected Honestly, the biggest reason is simple: It works. You take it, symptoms go away. You stop, they come back. So it feels like you need it. That doesn’t always mean long-term use is wrong. Sometimes it’s necessary. But sometimes it means: the underlying issue hasn’t been addressed lifestyle triggers are still there or something else is going on So instead of just continuing it indefinitely, it’s worth stepping back and figuring out the pattern. About long-term use (this is where people get concerned) Prilosec can be used long-term, but it’s not something doctors ignore. Over time, a few things can happen: your body may absorb less vitamin B12 magnesium levels can be affected there’s some concern about bone health with very long use possible links to kidney or gut-related issues Now — this doesn’t mean it’s unsafe. It just means that long-term use isn’t something you leave unreviewed. Doctors usually check: do you still need it? can the dose be lowered? can it be used less often? It’s about balance. Signs you probably shouldn’t just keep taking it There are certain patterns where it’s better not to just keep going with Prilosec on your own. Like if: symptoms come back quickly every time you stop you keep needing repeat 14-day courses heartburn doesn’t improve even after a full course symptoms feel different or worse than before That’s usually when it’s time to get proper advice instead of guessing. What actually helps reduce how long you need it This part gets overlooked a lot. Medication helps, but it’s not the whole solution. Things that can make a real difference: not eating heavy meals late at night avoiding trigger foods (spicy, acidic, fried) staying upright after eating weight management, if that’s a factor cutting back on alcohol or caffeine Even small changes here can reduce how much you rely on medication long-term. Realistically, how long do people take it? If we’re being honest, there’s a wide range. Some people: take it for 2 weeks and don’t need it again Others: take it for a couple of months And some: end up on it long-term, but under supervision So there’s no single answer that fits everyone. It depends on why you’re taking it in the first place. When you really shouldn’t wait it out There are a few symptoms where it’s better not to just keep taking Prilosec and hoping it settles. You should get checked if you notice: trouble swallowing unexplained weight loss persistent chest discomfort symptoms getting worse instead of better Those aren’t typical reflux patterns. One practical thing people don’t realize Stopping Prilosec can sometimes cause a temporary increase in acid (rebound effect). So symptoms might feel worse for a short time after stopping. That makes people think they still need it — even if the original issue improved. That’s another reason it helps to have a plan rather than stopping or restarting randomly. A quick, real-world note A lot of people end up taking Prilosec longer than they planned, mostly because it works well. But if you’re in that situation, it’s better to understand why you still need it instead of just continuing it indefinitely. If you’re unsure how long you should keep taking it, or whether it’s time to reduce or stop, a pharmacist at Sanford Pharmacy can walk through your situation with you. You can also check sanfordpharmacy.com if you want a clearer idea of how to use it safely over time. Prilosec is usually taken for about 14 days for simple heartburn, or several weeks for medical conditions. Longer use happens — but it should be intentional, not automatic.
Viral and Parasitic
How Long Does It Take Praziquantel to Kill Tapeworms?
Aaliya
08 May 2026
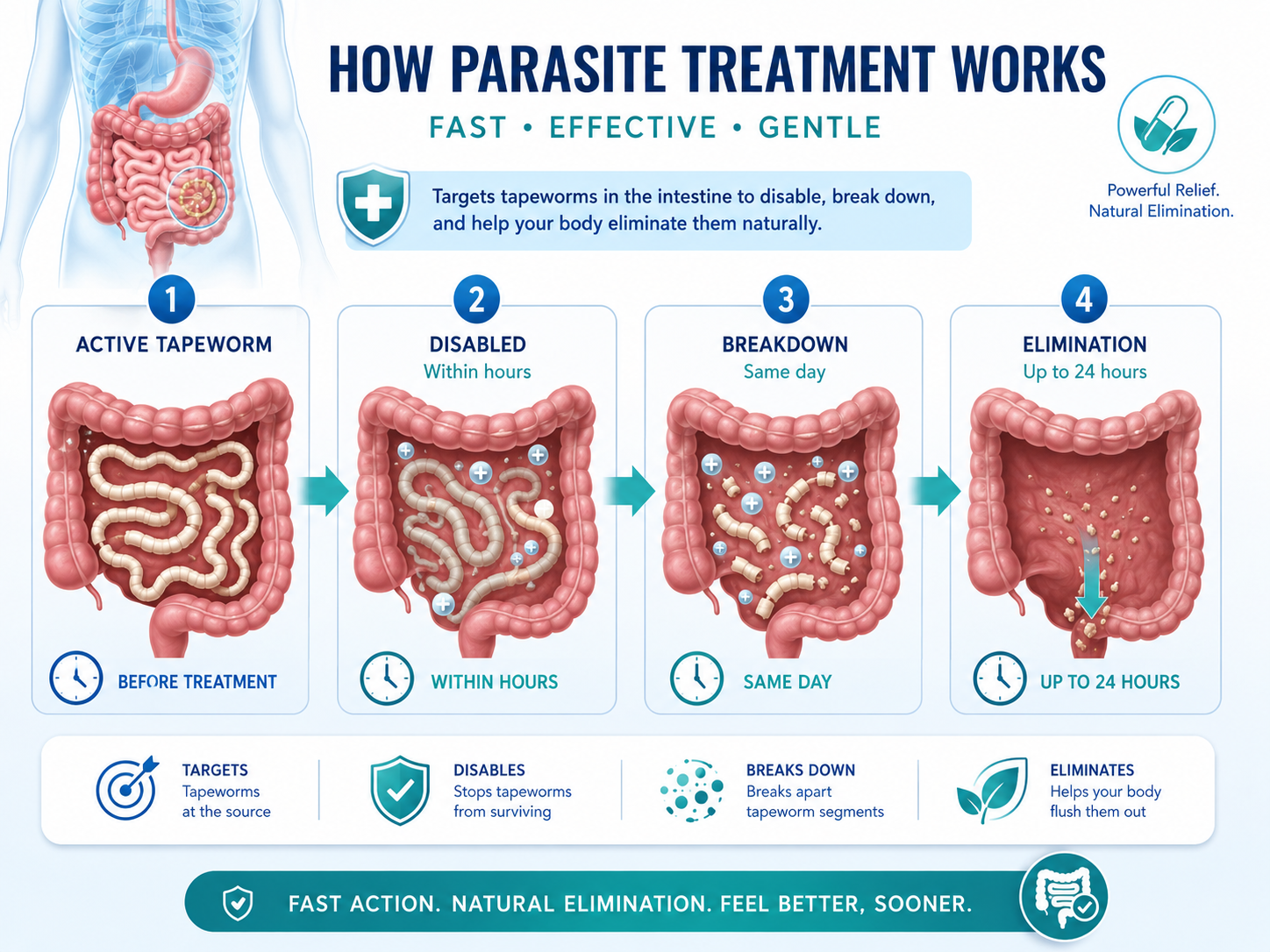
Praziquantel Treatment Timeline and Effectiveness for Tapeworm Infections Praziquantel works pretty fast. In most cases, it starts affecting tapeworms within a few hours after you take it, and the parasites are usually killed and begin clearing from your body within about 24 hours. Even though the drug acts quickly, your body might take a couple more days to fully get rid of everything. So the killing part is quick. The clearing part takes a little longer. How quickly praziquantel actually starts working This medication doesn’t sit around for days before doing anything. Once you take it, it gets absorbed and starts acting on the parasite fairly soon. People don’t usually “feel” it working, but biologically, things are already happening. it begins working within a few hours it disrupts the parasite’s structure pretty quickly in many cases, only one dose is needed That’s why praziquantel is often prescribed as a single-dose treatment for certain tapeworm infections. What actually happens to the tapeworm The process is a bit strange if you think about it, but here’s what’s going on. Praziquantel doesn’t just kill the worm instantly in one step. It affects how the parasite functions. After taking the medication: the tapeworm loses its grip on the intestinal wall it becomes paralyzed its outer structure gets damaged From there, your body takes over. The parasite either gets digested or passed out in stool. A lot of people expect to see the worm afterward, but in many cases, you don’t actually notice anything obvious. It can break down before you ever see it. How long it takes to fully clear the infection Even though praziquantel acts fast, your body still needs time to clean things up. most of the parasite is dealt with within 24 hours leftover material may take a few days to fully clear in some situations, follow-up testing is done to confirm it’s gone So while the medication does its job quickly, the full process isn’t always immediate. Why it might take longer for some people Not every infection behaves the same way. A few things can affect how quickly everything clears: the type of tapeworm involved how heavy the infection is the dose you were given your digestion and immune response In some cases, especially if the infection is more established, a second dose might be needed. That doesn’t mean the first one didn’t work — just that not everything cleared fully the first time. What you might feel after taking it Most people tolerate praziquantel fairly well, but you might notice a few things after taking it. Nothing severe in most cases, just mild effects like: slight abdominal discomfort nausea feeling a bit tired changes in bowel movements These are usually short-lived and settle as your body clears the infection. Sometimes the symptoms are related more to the parasite breaking down than the medication itself. When to check in with a doctor Even though treatment is usually straightforward, it’s still worth paying attention afterward. You should seek medical advice if: symptoms don’t improve you suspect the infection is still there side effects feel stronger than expected you’re told to follow up with testing It’s better to confirm everything has cleared rather than assume. A practical note Tapeworm treatment can feel a bit uncertain because you don’t always see clear signs that it’s gone. The medication does its job quietly in the background. If you’re unsure what to expect after taking praziquantel — or whether everything has cleared properly — a pharmacist at Sanford Pharmacy can help explain what’s normal and what isn’t. You can also check sanfordpharmacy.com for more guidance on treatment and follow-up. Praziquantel starts working within hours and usually kills tapeworms within a day. After that, your body takes a little more time to fully clear the remains, which is why the whole process can stretch over a couple of days.
Viral and Parasitic
How Long Does Acyclovir Stay in Your System?
Jayden
08 May 2026
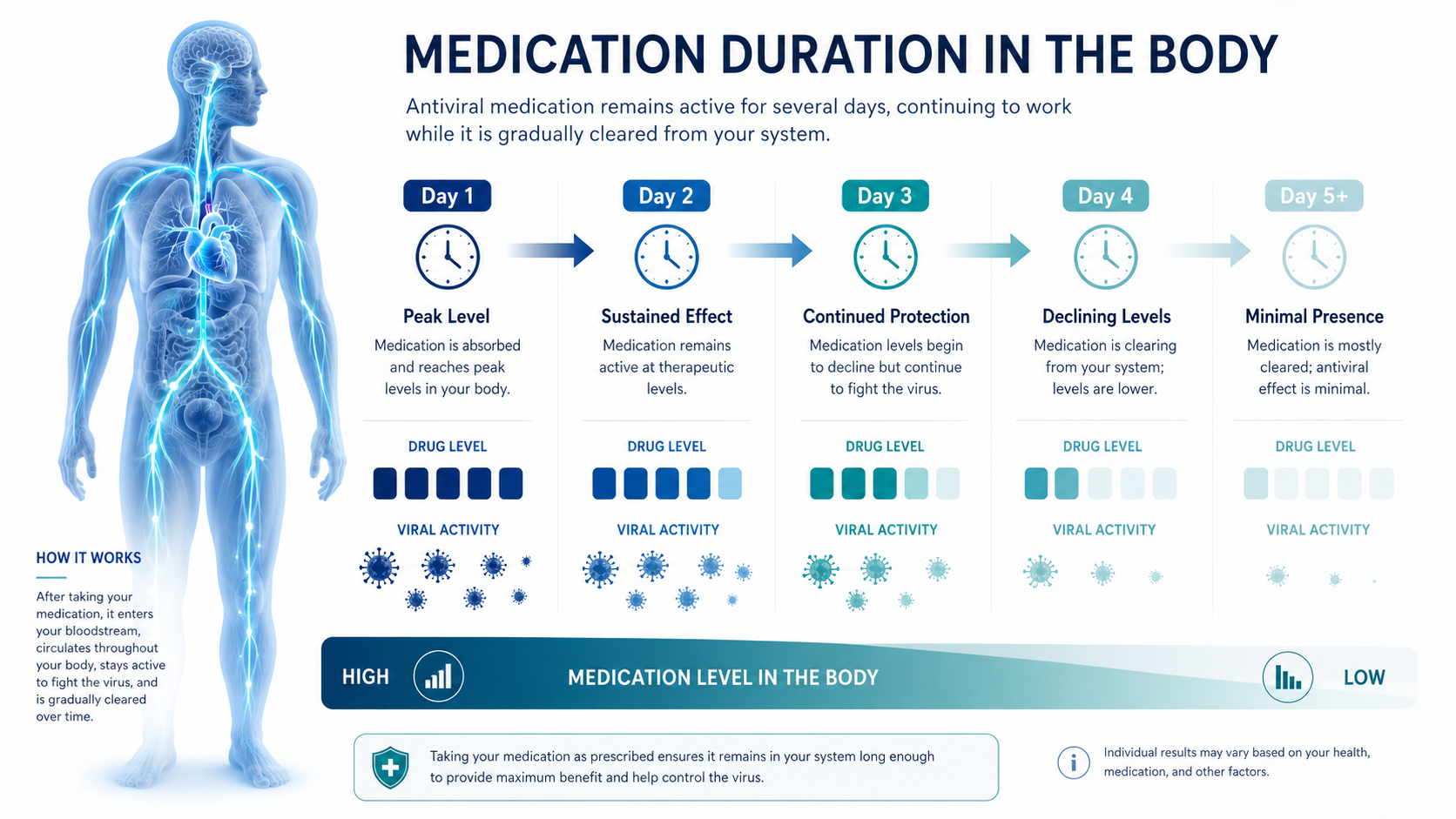
Understanding Antiviral Drug Duration and Clearance in the Body Acyclovir doesn’t hang around very long in the body compared to many other medications. In most healthy adults, it’s mostly cleared within about 10 to 20 hours after the last dose. Its half-life is only around 2.5 to 3 hours, so your body processes and removes it fairly quickly. That said, “cleared” doesn’t mean every last trace is gone instantly. Small amounts can linger a bit longer, especially depending on kidney function. What actually happens after you take acyclovir Once you take a dose, your body gets to work on it pretty quickly. Acyclovir is absorbed, does its job, and then starts getting filtered out — mainly through the kidneys. Here’s the general idea: half of the drug leaves your system in about 2.5–3 hours then half of what’s left goes again in the next few hours this keeps repeating until most of it is gone By the time you reach around 12 to 15 hours, most of the medication has been cleared. That’s why acyclovir is usually taken multiple times a day — it doesn’t stay at high levels for long. Why you might still hear “up to a day” Even though most of it clears in under a day, people often say it stays in your system for around 24 hours. That’s because: tiny amounts can still be present after the main clearance your body doesn’t eliminate everything at exactly the same speed lab-level traces can remain a bit longer So from a practical point of view, you can think of it as: main drug effect: gone within hours mostly cleared: within half a day fully out (including traces): about a day or so What affects how long it stays in your body Not everyone clears acyclovir at the same rate. A few factors can shift the timeline: kidney function – probably the biggest factor, since the drug is cleared through urine age – older adults may process it more slowly hydration – being well hydrated helps the kidneys do their job dose and how often you take it overall health and metabolism If kidney function is reduced, acyclovir can stay in the system longer than expected. That’s why dosing is sometimes adjusted in those cases. Does it keep working after it leaves your system? This part can feel a bit confusing. Acyclovir itself doesn’t stay active for very long, but the effect it has on the virus continues. It works by blocking viral replication — basically stopping the virus from multiplying. So even after levels drop: viral activity has already been slowed down your immune system continues clearing the infection symptoms can keep improving That’s why you might still feel better even after the drug levels are low. What happens after you stop taking it Once you stop acyclovir: most of the drug clears within about a day your body continues handling the infection symptoms may keep improving for a bit But in some cases, especially with conditions like herpes, the virus can reactivate later. That’s not because the drug is still there or not — it’s just how the virus behaves. Why it needs to be taken multiple times a day Because acyclovir leaves the body fairly quickly, it doesn’t maintain steady levels on its own. That’s why prescriptions often look like: 2 to 5 times daily dosing This keeps enough medication in your system throughout the day to stay effective. If doses are skipped or spaced too far apart, the level drops and the effect can weaken. When the timing actually matters For most people, you don’t need to think too much about how long it stays in your system. But it becomes more relevant if: you have kidney problems you’re experiencing side effects that seem to last longer you’re unsure about how often to take it you’re switching medications In those situations, understanding the timing helps avoid confusion. When to check with a professional It’s a good idea to get advice if: you have known kidney issues side effects continue after stopping the medication you’re unsure about dosing frequency symptoms aren’t improving as expected Sometimes it’s just about adjusting the schedule slightly. A practical note Acyclovir is one of those medications that works fast and leaves fast. That’s good in terms of safety and control, but it also means timing matters more than people expect. If you’re unsure how long it should stay in your system or how that affects your dosing, a pharmacist at Sanford Pharmacy can walk you through it based on your situation. You can also check sanfordpharmacy.com if you want a clearer idea of how to use antiviral medications properly. Acyclovir usually clears from the body within about a day, with most of it gone in the first 12–15 hours. It doesn’t stay long, but it does its job while it’s there.
How Long Can You Take Prilosec?
Mikayla
|
11 May 2026
How Long Does It Take Praziquantel to Kill Tapeworms?
Aaliya
|
08 May 2026
How Long Does Acyclovir Stay in Your System?
Jayden
|
08 May 2026

How Long Can You Use Tacrolimus Ointment?
Cheyenne
|
08 May 2026

How Long Does Zyrtec Stay in Your System?
Joseph Yajiv
|
08 May 2026
Recently Posted
Gastrointestinal and Metabolic
How Long Can You Take Prilosec?
Mikayla
11 May 2026
Safe Duration and Long-Term Use of Proton Pump Inhibitors Explained Prilosec isn’t really meant to be something you just take forever without thinking about it. For most people, it’s used for a short stretch — about 14 days if you’re taking it over the counter. If it’s prescribed, that can stretch to 4 to 8 weeks, sometimes longer depending on what’s going on. But the key thing is — the longer you stay on it, the more it should be something you’re checking with a doctor or pharmacist about, not just continuing on your own. What “14 days” actually means (because people misunderstand this a lot) If you look at the box, it says 14 days. Sounds simple. But here’s what that really means in practice: you take it once a day, every day for the full 14 days you don’t just stop when you feel better after a couple days and it’s not something you’re supposed to restart immediately again and again A lot of people take it for 3–4 days, feel better, and stop. Then symptoms come back. That’s because Prilosec doesn’t work like an instant antacid. It builds up its effect. It usually takes a few days (sometimes up to 4) before you feel the full benefit. So the 14 days is more about giving it time to properly settle things down. What happens if symptoms come back This is where things get tricky for a lot of people. You finish the 14 days… and then a week later, heartburn is back. So you take another course. Then maybe another. At that point, it’s less about “how long can I take it” and more about “why do I need it this often?” If you’re repeating those 14-day cycles regularly, it’s usually a sign something needs a closer look. When people are told to take it longer There are definitely situations where Prilosec is used for more than just two weeks. Doctors prescribe it longer for things like: GERD (chronic acid reflux) stomach ulcers duodenal ulcers H. pylori infections (along with antibiotics) In those cases, it’s often: 4 to 8 weeks sometimes longer if symptoms don’t fully settle And sometimes people stay on a lower dose after that. But again — that’s usually planned and monitored, not just continued casually. Why people end up staying on it longer than expected Honestly, the biggest reason is simple: It works. You take it, symptoms go away. You stop, they come back. So it feels like you need it. That doesn’t always mean long-term use is wrong. Sometimes it’s necessary. But sometimes it means: the underlying issue hasn’t been addressed lifestyle triggers are still there or something else is going on So instead of just continuing it indefinitely, it’s worth stepping back and figuring out the pattern. About long-term use (this is where people get concerned) Prilosec can be used long-term, but it’s not something doctors ignore. Over time, a few things can happen: your body may absorb less vitamin B12 magnesium levels can be affected there’s some concern about bone health with very long use possible links to kidney or gut-related issues Now — this doesn’t mean it’s unsafe. It just means that long-term use isn’t something you leave unreviewed. Doctors usually check: do you still need it? can the dose be lowered? can it be used less often? It’s about balance. Signs you probably shouldn’t just keep taking it There are certain patterns where it’s better not to just keep going with Prilosec on your own. Like if: symptoms come back quickly every time you stop you keep needing repeat 14-day courses heartburn doesn’t improve even after a full course symptoms feel different or worse than before That’s usually when it’s time to get proper advice instead of guessing. What actually helps reduce how long you need it This part gets overlooked a lot. Medication helps, but it’s not the whole solution. Things that can make a real difference: not eating heavy meals late at night avoiding trigger foods (spicy, acidic, fried) staying upright after eating weight management, if that’s a factor cutting back on alcohol or caffeine Even small changes here can reduce how much you rely on medication long-term. Realistically, how long do people take it? If we’re being honest, there’s a wide range. Some people: take it for 2 weeks and don’t need it again Others: take it for a couple of months And some: end up on it long-term, but under supervision So there’s no single answer that fits everyone. It depends on why you’re taking it in the first place. When you really shouldn’t wait it out There are a few symptoms where it’s better not to just keep taking Prilosec and hoping it settles. You should get checked if you notice: trouble swallowing unexplained weight loss persistent chest discomfort symptoms getting worse instead of better Those aren’t typical reflux patterns. One practical thing people don’t realize Stopping Prilosec can sometimes cause a temporary increase in acid (rebound effect). So symptoms might feel worse for a short time after stopping. That makes people think they still need it — even if the original issue improved. That’s another reason it helps to have a plan rather than stopping or restarting randomly. A quick, real-world note A lot of people end up taking Prilosec longer than they planned, mostly because it works well. But if you’re in that situation, it’s better to understand why you still need it instead of just continuing it indefinitely. If you’re unsure how long you should keep taking it, or whether it’s time to reduce or stop, a pharmacist at Sanford Pharmacy can walk through your situation with you. You can also check sanfordpharmacy.com if you want a clearer idea of how to use it safely over time. Prilosec is usually taken for about 14 days for simple heartburn, or several weeks for medical conditions. Longer use happens — but it should be intentional, not automatic.
Viral and Parasitic
How Long Does It Take Praziquantel to Kill Tapeworms?
Aaliya
08 May 2026
Praziquantel Treatment Timeline and Effectiveness for Tapeworm Infections Praziquantel works pretty fast. In most cases, it starts affecting tapeworms within a few hours after you take it, and the parasites are usually killed and begin clearing from your body within about 24 hours. Even though the drug acts quickly, your body might take a couple more days to fully get rid of everything. So the killing part is quick. The clearing part takes a little longer. How quickly praziquantel actually starts working This medication doesn’t sit around for days before doing anything. Once you take it, it gets absorbed and starts acting on the parasite fairly soon. People don’t usually “feel” it working, but biologically, things are already happening. it begins working within a few hours it disrupts the parasite’s structure pretty quickly in many cases, only one dose is needed That’s why praziquantel is often prescribed as a single-dose treatment for certain tapeworm infections. What actually happens to the tapeworm The process is a bit strange if you think about it, but here’s what’s going on. Praziquantel doesn’t just kill the worm instantly in one step. It affects how the parasite functions. After taking the medication: the tapeworm loses its grip on the intestinal wall it becomes paralyzed its outer structure gets damaged From there, your body takes over. The parasite either gets digested or passed out in stool. A lot of people expect to see the worm afterward, but in many cases, you don’t actually notice anything obvious. It can break down before you ever see it. How long it takes to fully clear the infection Even though praziquantel acts fast, your body still needs time to clean things up. most of the parasite is dealt with within 24 hours leftover material may take a few days to fully clear in some situations, follow-up testing is done to confirm it’s gone So while the medication does its job quickly, the full process isn’t always immediate. Why it might take longer for some people Not every infection behaves the same way. A few things can affect how quickly everything clears: the type of tapeworm involved how heavy the infection is the dose you were given your digestion and immune response In some cases, especially if the infection is more established, a second dose might be needed. That doesn’t mean the first one didn’t work — just that not everything cleared fully the first time. What you might feel after taking it Most people tolerate praziquantel fairly well, but you might notice a few things after taking it. Nothing severe in most cases, just mild effects like: slight abdominal discomfort nausea feeling a bit tired changes in bowel movements These are usually short-lived and settle as your body clears the infection. Sometimes the symptoms are related more to the parasite breaking down than the medication itself. When to check in with a doctor Even though treatment is usually straightforward, it’s still worth paying attention afterward. You should seek medical advice if: symptoms don’t improve you suspect the infection is still there side effects feel stronger than expected you’re told to follow up with testing It’s better to confirm everything has cleared rather than assume. A practical note Tapeworm treatment can feel a bit uncertain because you don’t always see clear signs that it’s gone. The medication does its job quietly in the background. If you’re unsure what to expect after taking praziquantel — or whether everything has cleared properly — a pharmacist at Sanford Pharmacy can help explain what’s normal and what isn’t. You can also check sanfordpharmacy.com for more guidance on treatment and follow-up. Praziquantel starts working within hours and usually kills tapeworms within a day. After that, your body takes a little more time to fully clear the remains, which is why the whole process can stretch over a couple of days.
Viral and Parasitic
How Long Does Acyclovir Stay in Your System?
Jayden
08 May 2026
Understanding Antiviral Drug Duration and Clearance in the Body Acyclovir doesn’t hang around very long in the body compared to many other medications. In most healthy adults, it’s mostly cleared within about 10 to 20 hours after the last dose. Its half-life is only around 2.5 to 3 hours, so your body processes and removes it fairly quickly. That said, “cleared” doesn’t mean every last trace is gone instantly. Small amounts can linger a bit longer, especially depending on kidney function. What actually happens after you take acyclovir Once you take a dose, your body gets to work on it pretty quickly. Acyclovir is absorbed, does its job, and then starts getting filtered out — mainly through the kidneys. Here’s the general idea: half of the drug leaves your system in about 2.5–3 hours then half of what’s left goes again in the next few hours this keeps repeating until most of it is gone By the time you reach around 12 to 15 hours, most of the medication has been cleared. That’s why acyclovir is usually taken multiple times a day — it doesn’t stay at high levels for long. Why you might still hear “up to a day” Even though most of it clears in under a day, people often say it stays in your system for around 24 hours. That’s because: tiny amounts can still be present after the main clearance your body doesn’t eliminate everything at exactly the same speed lab-level traces can remain a bit longer So from a practical point of view, you can think of it as: main drug effect: gone within hours mostly cleared: within half a day fully out (including traces): about a day or so What affects how long it stays in your body Not everyone clears acyclovir at the same rate. A few factors can shift the timeline: kidney function – probably the biggest factor, since the drug is cleared through urine age – older adults may process it more slowly hydration – being well hydrated helps the kidneys do their job dose and how often you take it overall health and metabolism If kidney function is reduced, acyclovir can stay in the system longer than expected. That’s why dosing is sometimes adjusted in those cases. Does it keep working after it leaves your system? This part can feel a bit confusing. Acyclovir itself doesn’t stay active for very long, but the effect it has on the virus continues. It works by blocking viral replication — basically stopping the virus from multiplying. So even after levels drop: viral activity has already been slowed down your immune system continues clearing the infection symptoms can keep improving That’s why you might still feel better even after the drug levels are low. What happens after you stop taking it Once you stop acyclovir: most of the drug clears within about a day your body continues handling the infection symptoms may keep improving for a bit But in some cases, especially with conditions like herpes, the virus can reactivate later. That’s not because the drug is still there or not — it’s just how the virus behaves. Why it needs to be taken multiple times a day Because acyclovir leaves the body fairly quickly, it doesn’t maintain steady levels on its own. That’s why prescriptions often look like: 2 to 5 times daily dosing This keeps enough medication in your system throughout the day to stay effective. If doses are skipped or spaced too far apart, the level drops and the effect can weaken. When the timing actually matters For most people, you don’t need to think too much about how long it stays in your system. But it becomes more relevant if: you have kidney problems you’re experiencing side effects that seem to last longer you’re unsure about how often to take it you’re switching medications In those situations, understanding the timing helps avoid confusion. When to check with a professional It’s a good idea to get advice if: you have known kidney issues side effects continue after stopping the medication you’re unsure about dosing frequency symptoms aren’t improving as expected Sometimes it’s just about adjusting the schedule slightly. A practical note Acyclovir is one of those medications that works fast and leaves fast. That’s good in terms of safety and control, but it also means timing matters more than people expect. If you’re unsure how long it should stay in your system or how that affects your dosing, a pharmacist at Sanford Pharmacy can walk you through it based on your situation. You can also check sanfordpharmacy.com if you want a clearer idea of how to use antiviral medications properly. Acyclovir usually clears from the body within about a day, with most of it gone in the first 12–15 hours. It doesn’t stay long, but it does its job while it’s there.
Dermatology and Topical Treatments
How Long Can You Use Tacrolimus Ointment?
Cheyenne
08 May 2026
Safe Duration and Long-Term Use of Tacrolimus Ointment for Skin Conditions Tacrolimus ointment can be used for short periods during flare-ups and also off and on over the long term, depending on your skin condition and how your doctor wants you to use it. Most people apply it daily when symptoms are active, then reduce or stop once things calm down. In some cases, it’s used a few times a week long-term to help keep flare-ups from coming back. So it’s not just a “use for 7 days and stop” kind of medication. The timing can change based on how your skin behaves. How long people usually use it during flare-ups When symptoms are active — like eczema flaring up — tacrolimus is usually used more regularly. Typical pattern looks like this: applied twice a day on affected areas continued until the skin improves or clears this can take a few days… or a few weeks There’s no exact number of days that fits everyone. Some people respond quickly. Others need a bit longer before things settle down. Once the redness, itching, and irritation calm down, the usual step is to reduce how often you’re using it rather than just continuing the same routine. What happens after the skin improves This is where tacrolimus is a bit different from some other treatments. You don’t always stop it completely right away. Instead, many people shift to a lighter schedule, like: using it 2–3 times a week applying it only on areas that tend to flare This is often called maintenance use. The idea is to keep the skin stable and prevent another flare, instead of waiting for symptoms to come back and starting over again. Why it can be used longer than steroid creams A big reason tacrolimus gets used this way is because it doesn’t have some of the limitations that topical steroids do. For example: it doesn’t thin the skin it’s safer for sensitive areas like the face, eyelids, or neck it can be used repeatedly over time without the same risks That’s why it’s often chosen for long-term skin conditions like eczema (atopic dermatitis), where symptoms tend to come and go. How you know when to reduce or stop There’s usually a point where you’ll notice the skin looks and feels better. That’s the signal to adjust. You might be advised to reduce or pause use when: the skin is mostly clear itching has settled down redness is minimal or gone At that stage, continuing twice daily isn’t always needed. But it’s still important to follow what your doctor suggested, because stopping too early or too suddenly can sometimes lead to flare-ups coming back quickly. Why the duration isn’t the same for everyone There’s no single timeline for tacrolimus. How long you use it depends on a few things: how severe the condition is how often flare-ups happen how your skin responds where on the body you’re using it Some people only need it occasionally. Others end up using it regularly (but not daily) over longer periods to keep things under control. Both situations are common. Things to keep in mind with longer use Tacrolimus is generally considered safe when used as directed, but there are still a few practical things to be aware of. apply it only to the areas that need it avoid using it continuously every single day for long periods unless advised try to protect treated skin from too much sun exposure mild burning or warmth can happen at first — that usually settles If you’re using it over a longer period, occasional check-ins with a healthcare provider are usually recommended just to make sure everything is on track. When it’s worth asking for advice It’s a good idea to check in if: symptoms aren’t improving after a few weeks irritation or burning doesn’t settle flare-ups keep coming back quickly you’re unsure how often you should continue using it Sometimes the treatment plan just needs a small adjustment. A practical note Tacrolimus isn’t a “one schedule fits everyone” type of treatment. It’s more flexible than that, which is helpful — but also a bit confusing if you’re trying to figure it out on your own. If you’re unsure how long you should keep using it or when to switch to a maintenance routine, a pharmacist at Sanford Pharmacy can help you go through it step by step. You can also check sanfordpharmacy.com for guidance on how to use it safely and consistently. Tacrolimus ointment is usually used daily during flare-ups, then reduced or used occasionally over the longer term. The exact duration depends on how your skin responds and how often symptoms come back.
Allergy and Immunology
How Long Does Zyrtec Stay in Your System?
Joseph Yajiv
08 May 2026
Cetirizine Duration, Half-Life, and Clearance in the Body Explained Zyrtec stays in your system for about 2 to 3 days after your last dose, even though you only feel its effects for around 24 hours. The medication doesn’t just disappear once it stops working — it fades out slowly as your body clears it over time. That’s where people get confused. Feeling better and the drug leaving your body are two different things. How long the effects actually last For most people, Zyrtec is a once-a-day medication. You take it, and: it controls symptoms for about 24 hours you don’t usually need another dose during that time it covers both day and night symptoms So in terms of how it feels, it’s pretty straightforward — one dose, one full day of relief. But after that relief wears off, the medication itself is still there in smaller amounts. What’s happening in the body after you take it Once you take Zyrtec, your body absorbs it and then starts breaking it down. This doesn’t happen all at once. Zyrtec has something called a half-life, which is basically how long it takes for half of the drug to leave your system. For cetirizine (Zyrtec), that’s about 8 hours in most healthy adults. So what happens is: after 8 hours, about half is gone after another 8 hours, half of what’s left is gone and so on It keeps reducing in steps. It usually takes about 5 of these cycles for most of the drug to clear out. That comes out to roughly 40 hours, sometimes a bit longer. And then there can still be tiny traces hanging around after that — which is why people say 2 to 3 days overall. Why it doesn’t feel like it’s still there Even though Zyrtec stays in your system for a couple of days, you don’t feel it the whole time. That’s because: the level in your body drops below what’s needed to control symptoms the remaining amount isn’t strong enough to have a noticeable effect So from your perspective, it “stopped working” after a day. But from a pharmacology standpoint, it’s still clearing out. What can change how long it stays Not everyone processes medication the same way. There are a few things that can make Zyrtec stay in your system a bit longer or shorter: age — older adults may clear it more slowly kidney function — this is a big one, since the drug is cleared through the kidneys dose and how often you take it overall metabolism and health If kidney function is reduced, the medication can stay in the body longer than expected. That’s why dosing sometimes needs adjustment in those cases. Does it build up if you take it every day? This is something people often wonder about. If you take Zyrtec daily, it can reach what’s called a steady level in your body. That just means: you’re taking it at about the same rate your body is clearing it the amount in your system stays fairly stable It doesn’t keep building up endlessly. When taken as directed, it doesn’t usually reach harmful levels. Instead, it helps keep allergy symptoms under control consistently. What happens when you stop taking it Once you stop Zyrtec, two things happen at the same time. First, the effects wear off: allergy symptoms may start coming back within 24 to 48 hours Second, the drug continues clearing out: levels gradually drop over the next couple of days no tapering is needed — you can just stop There’s no “withdrawal” in the usual sense, but symptoms returning can make it feel like something changed suddenly. When this actually matters For most people, knowing how long Zyrtec stays in the system isn’t something they need to think about every day. But it becomes more relevant if: you’re switching to another allergy medication you have kidney issues you’re dealing with side effects that seem to last longer than expected you’re trying to understand why symptoms came back In those situations, timing matters a bit more. When to ask someone about it It’s worth checking with a healthcare professional if: you have known kidney problems side effects seem to last longer than they should you’re unsure about dosing or switching medications Sometimes it’s just a small adjustment that makes things clearer. A practical note It’s easy to assume that once a medication “stops working,” it’s out of your system. But with Zyrtec, that’s not really how it works. It continues to clear slowly in the background. If you’re unsure how that affects your dosing or timing — especially if you’re taking other medications — a pharmacist at Sanford Pharmacy can help explain it in a way that fits your situation. You can also check sanfordpharmacy.com if you want more guidance on how to manage allergy medications safely. Zyrtec usually works for about a day, but stays in your system for a couple of days after that. The effect fades first — the medication itself takes longer to fully leave.

Allergy and Immunology
How Long Does Zyrtec Take to Work?
Hana
08 May 2026
Zyrtec Onset Time, Duration, and Allergy Relief Guide Zyrtec usually starts working within about 20 to 60 minutes, and most people feel some relief within an hour. For some people the effects begin to show even sooner than that. The medication begins to work after intake and provides effects that last for 24 hours which explains its common usage as a single daily dose. It’s not instant like a nasal spray, but it’s still pretty fast for an oral allergy tablet. What it feels like when it starts working It doesn’t hit all at once. Usually, the first thing people notice is that symptoms feel a bit less intense. Not gone — just easier. Sneezing slows down. The constant itch settles a bit. Your nose isn’t running as much. That can start as early as 20–30 minutes for some people. By around the 1-hour mark, most people can clearly tell it’s doing something. After that, it continues to build for a bit before leveling out. How long it keeps working One of the main reasons people like Zyrtec is how long it lasts. it works for up to 24 hours usually taken once daily covers both daytime and nighttime symptoms So once it’s in your system, you’re generally covered for the whole day. You don’t have to keep taking doses every few hours like older antihistamines. Why it feels fast for some people Not everyone experiences it the same way. Some people say it works really quickly. Others feel like it takes closer to an hour. That depends on a few things: your metabolism how strong your symptoms are whether you took it before or after exposure how your body reacts to antihistamines For mild occurrence, you will feel relief sooner. It may take a little longer before you begin to feel a distinct difference if the symptoms are more intense. What symptoms it actually helps with Zyrtec works best for symptoms caused by histamine — which is basically what your body releases during an allergic reaction. So it helps with things like: sneezing runny nose itchy or watery eyes itching in the nose or throat hives It’s not as strong for nasal congestion compared to some other treatments, but for itching and sneezing, it’s usually pretty effective. Why taking it daily makes a difference A lot of people take Zyrtec only when symptoms show up. It still works that way. But it often works better when taken regularly during allergy season. When you take it daily: it keeps histamine levels more controlled symptoms are less likely to spike overall relief feels more consistent So instead of reacting to symptoms, you’re staying ahead of them. Small things that can affect how fast it works There are a few simple factors that can change how quickly you feel it: taking it at the same time each day helps keep levels steady taking it before allergen exposure can make it feel faster skipping doses can make it feel less effective your body’s sensitivity to medication plays a role Sometimes people think it “stopped working,” but it’s really just inconsistent use. When it might not feel like enough If Zyrtec doesn’t seem to be helping, it doesn’t always mean it’s the wrong medication — but it might need adjusting. You might notice: symptoms not improving after a few days relief that feels partial, not complete ongoing irritation despite taking it At that point, it’s worth checking whether: the timing is right something else (like congestion) needs a different treatment another medication might work better When to check with someone It’s a good idea to speak with a healthcare professional if: symptoms don’t improve after a few days you feel unusually drowsy you’re not sure if it’s the right medication for your symptoms allergies feel more severe than usual Sometimes a small change makes a big difference. A quick practical note Zyrtec is one of those medications that works fairly quickly, but it’s still easy to misjudge it based on one dose. If you need help understanding the correct timing and dosage for optimal results, speaking to someone who understands your situation will assist you better. A pharmacist at Sanford Pharmacy can help you figure out the best timing and whether Zyrtec fits your symptoms. You can visit sanfordpharmacy.com to obtain detailed information about correct usage and expected outcomes. Zyrtec usually starts working within an hour and keeps going for a full day. For most people, it’s quick enough to notice and long enough to rely on.
Popular Medicines
.webp)
.webp)
-(2).webp)

.webp)
.webp)
.webp)
.webp)
_1.webp)

-(1).webp)
.webp)
.webp)








Free Airmail Shipping Anywhere in USA